Shoulder Tendinitis
Shoulder Tendinitis, Bursitis, and Impingement
Shoulder pain is a common occurrence for athletes and people in general. A sudden traumatic injury to the shoulder, such as a fracture or dislocation, requires immediate medical attention. The athlete should contact his physician or go to the emergency room as soon as possible. Shoulder dislocations commonly occur in football, basketball, and snowboarding. Overuse or wear-and-tear injuries, instability problems, strains, and sprains are common in throwing and overhead sports such as baseball, volleyball, basketball, water polo, and swimming. Shoulder tendinitis, bursitis, and impingement are among the most common overuse injuries of the shoulder. The pain is usually felt at the tip of the shoulder and down the upper arm. The pain occurs when the arm is lifted overhead or twisted. As the shoulder inflammation becomes more severe, the pain will be present all the time, and it may even wake the athlete from a deep sleep.
Anatomy
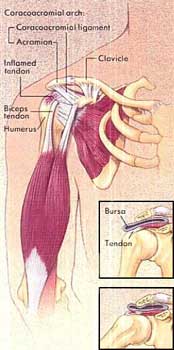
The shoulder is a closely fitted joint. The humerus (upper arm bone), certain muscle tendons, and associated bursa (fluid-filled sacs that cushion bone to prevent friction), move back and forth through a very tight archway of bone and ligament called the coracoacromial arch. When the arm is raised, the archway becomes smaller, pinches the tendons, and can cause inflammation of the tissues. Pinching or impingement of the rotator cuff tendons can lead to tendinitis. If there is prolonged impingement, the rotator cuff tendon cuff can actually tear. Shoulder bursa can become inflamed and painful as surrounding muscles move over them, causing bursitis. Symptoms of shoulder tendonitis and bursitis, such as pain, swelling, stiffness, and weakness can last for a few days, recur, or become chronic.
Contributing Factors
- Overuse. This is the result of repetitive overhead motions is the most common cause of shoulder tendinitis, bursitis, and impingement.
- Weak muscles. When the muscles are weak, more force is exerted on the tendons and bursa, causing inflammation and pain.
- Improper or inappropriate swimming or throwing techniques.
- Strenuous training. One hard throw, overhead serve, or swim stroke may start the problem.
- Previous injuries to the shoulder.
- Loose shoulder joint. In the teens and early twenties, the most common shoulder injuries are due to joint instability. An unstable shoulder can be the result of how the joint developed or from a strong force that caused the shoulder to dislocate or sublux. A shoulder subluxation injury results in a milder amount of instability where the ball slips partially out of its socket.
- Calcium deposits.
- Impingement. The shape of the bones that form the archway of the shoulder or degenerative changes of these bones (bone spurs), which are the result of wear-and-tear, can cause narrowing and pinching of the rotator cuff tendons.
Treatment
- Rest. Avoid activities that make the shoulder pain worse and caused the pain in the first place. The opposite shoulder and all other joints can still be exercised.
- Ice. Ice (e.g., a bag of ice) can be applied to the shoulder for 20 – 30 minutes, 3 – 4 times per day initially and then 2 times per day. Apply ice for 15 minutes after any activity involving the shoulder to minimize additional inflammation caused by the activity. Ice massage is a very effective form of ice application.
- Exercises. Stretching exercises of the shoulder and arm are essential to help improve muscle tendon flexibility and strength. These exercises help reverse the muscle weakness which results from the inflammation and enable the tendons to resume the usual demands and workloads of the sport (see section on Exercises).
- Physical Therapy. This may be necessary to help reduce the shoulder inflammation. The physical therapist may use such modalities as ultrasound, phonophoresis, iontophoresis, friction massage, electrogalvanic stimulation, and soft tissue mobilization to treat scar tissue in the tendons caused by the chronic inflammation.
- Medication. An oral anti-inflammatory may be prescribed or recommended. A shoulder injection of cortisone and a local anesthetic may be advised. The injection can help relieve the pain and tenderness and make physical therapy more effective. After an injection, the athlete should avoid return to sports for one to two weeks. A successful injection can often spare the need for surgery. Repeated injections should be avoided.
- Surgery. Sometimes surgery is required to treat this condition. If shoulder impingement cannot be relieved and if bone spurs and calcium deposits are a likely cause, then surgery may be necessary to correct these problems. In most cases, arthroscopic surgery of the shoulder will be performed, requiring a limited number of small incisions and done as a same-day surgery. Certain injuries, such as complete tears of the rotator cuff, often require surgical reconstruction.
Diagnosing Shoulder Problems
In the majority of cases, the sports medicine physician can diagnose a shoulder injury with a thorough medical history and a comprehensive physical exam. There are more than 50 shoulder exam tests that the physician can perform, each one providing specific clues about the nature of the shoulder injury. The physician may order additional tests, such as X-rays, MRI scan, and arthrogram, to provide him with more information and assist him in the diagnosis. Time is an important component in the diagnosis and treatment of shoulder problems. Some shoulder injuries take a long time to heal, sometimes weeks to months. The diagnosis of "little league shoulder," which is a stress reaction in the growth plate of the shoulder joint similar to a fracture, requires that the child stop throwing until the area heals completely.
Returning to Sports
Warming Up. The athlete should move all major joints through their complete range of motion several times before starting play. Stretching and strengthening exercises help prevent injury.
Playing the Game. When resuming the sport of choice, play at a lower intensity. In tennis, plan to rally for a short period of time and avoid difficult, problem shots. Play for a lesser amount of time or play doubles. Resume competitive play once the shoulder is healed.
Throwing Sports. Initially, an underhand or sidearm throw will be easier than an overhand throw. Warm up well. Throw easily and gradually increase to harder throwing. Start with the short-toss drill and gradually lengthen the throw. If there is no pain in the shoulder with the short toss, then begin the long-toss drill. Try to maintain a smooth throwing motion. When throwing, the athlete should rely more on his overall body strength, which will relieve some of the workload on his shoulder. Taking pitching lessons from a local pro can help with technique, form, and eliminate flaws.
Swimming. The breaststroke or side stroke will be easier to do initially than the front crawl, freestyle, or butterfly strokes. Sometimes the backstroke causes less pain. The athlete should do swim sprints early in his workout before he is fatigued. Consulting a swim coach may be necessary to help make changes in the stroke, swimming or diving style, thus improving performance and preventing future shoulder problems.
Exercises
Range of motion (ROM) exercises must be done twice daily to keep the joints mobile. These exercises consist of moving the joint carefully, as far as it can go in all directions. After the pain has subsided, shoulder muscles must be strengthened to prevent tendinitis, bursitis, and impingement from recurring. Do each prescribed exercise two times a day or more often if necessary.
Range-of-Motion Exercises
Start with the "pendulum swing." Support yourself with your healthy arm as shown. Keeping your knees slightly bent, bend forward at the waist and let your injured arm hang down (or dangle from the bed). Then make circles with your arm, first in a clockwise, then in a counter-clockwise direction. Start with small circles and gradually make them larger. Add the criss-cross ROM exercise by moving your arm in a vertical direction, then in a horizontal direction. Repeat each exercise 50 times, and do 2 times/day.

With palm out, place the hand of your injured arm behind your back and reach up as high as possible as though you were going to scratch your back with your thumb. Repeat 15 times, 2 times/day.

The back portion of the shoulder joint can be stretched out in this position by gently pulling your arm across your body as shown. Repeat 15 times, 2 times/day.

Standing with arms close to your body and elbows bent to 90 degrees, hands pointing straight ahead, slowly move arms so that hands point out to the side. Lower your arms to your sides, then raise the injured arm overhead as shown, helping with your other hand. Repeat 15 times, 2 times/day.

Strengthening Exercises
Exercises With Weights or Resistance. These exercises can be done with cans of food, three- and five- pound dumbbell weights, or stretchable tubing or cord, available from medical-supply and sporting-goods stores. See examples of hand weights, wrist weights, and TheraBand tubing and bands in the Sports Med Store. Avoid raising arms above shoulder level. Biceps and triceps exercises may also be done with weights.
With elbows straight, thumbs turned toward floor, and arms about 30 degrees forward, slowly raise arms to just below shoulder level. Slowly lower arms to starting position and repeat.

Lie on your side as shown with injured shoulder up, holding elbow close against ribs. Slowly raise weight until it points to ceiling. Then lower to starting position. Repeat 10 times, 2 times/day.

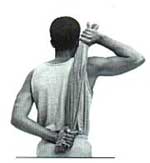
Stretching. Behind your back, hold one end of a towel with your good arm at shoulder level, as shown. Hold the other end with injured arm. Raise towel with good arm as high as you can without pain. Hold five seconds, slowly lower, relax, and repeat. Repeat 15 times, 2 times/day.
I cannot give medical advice about how to treat a specific injury without evaluating the athlete first. While I may discuss general exercises to prevent and treat sports injuries, not all exercises are designed for all individuals or problems. A sports medicine physician should be consulted before starting any exercise program. If an athlete is experiencing any severe pain or discomfort, he should see such a physician and obtain a specific diagnosis and treatment plan. The exercises outlined here are general recommendations and are not intended as a substitute for professional medical advice.
Specialty Reference
Shoulder Center